
Page 28 - Practical Approaches to Managing Castration-Resistant Prostate Cancer (CRPC)
P. 28
Androgen Deprivation Therapy
• The androgen receptor remains active in most patients with CRPC
• Continue ADT to maintain castrate levels of testosterone (for the duration of the
patient’s life)
ARAT (Androgen Receptor Axis-Targeted)
Agents
®
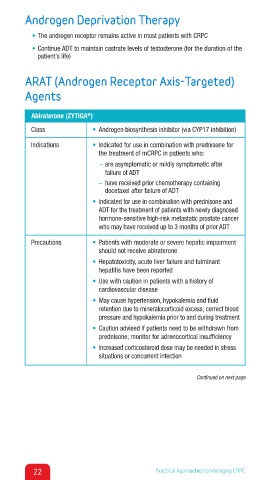
Abiraterone (ZYTIGA )
Class • Androgen biosynthesis inhibitor (via CYP17 inhibition)
Indications • Indicated for use in combination with prednisone for
the treatment of mCRPC in patients who:
– are asymptomatic or mildly symptomatic after
failure of ADT
– have received prior chemotherapy containing
docetaxel after failure of ADT
• Indicated for use in combination with prednisone and
ADT for the treatment of patients with newly diagnosed
hormone-sensitive high-risk metastatic prostate cancer
who may have received up to 3 months of prior ADT
Precautions • Patients with moderate or severe hepatic impairment
should not receive abiraterone
• Hepatotoxicity, acute liver failure and fulminant
hepatitis have been reported
• Use with caution in patients with a history of
cardiovascular disease
• May cause hypertension, hypokalemia and fluid
retention due to mineralocorticoid excess; correct blood
pressure and hypokalemia prior to and during treatment
• Caution advised if patients need to be withdrawn from
prednisone; monitor for adrenocortical insufficiency
• Increased corticosteroid dose may be needed in stress
situations or concurrent infection
Continued on next page
22 Practical Approaches to Managing CRPC